Myopia Progression
For many, it’s a familiar cycle:
Distance vision gets a bit blurry.
Eye doctor prescribes glasses: Your distance vision through the lenses looks nice and sharp!
Every morning, you put the glasses on, and go about your day, viewing everything through the updated prescription.
A few months go by, and you may begin to notice that by the end of the day, the distance may be a bit blurry.
Maybe it’s transient: You blink a few times, and the vision clears up.
- As a kid, you notice this on the chalkboard, especially if you’re seated near the back of the room.
- As a young adult, it’s the drive home that makes you wonder if your vision is fully corrected…
So… you take a trip back to the eye doctor.
“Yes, indeed…! Your vision has changed ‘just a bit,’ and you will see better when you get your glasses updated.”
The eye doctor prescribes new lenses, and once again, your distance vision — through the lenses— looks nice and sharp!
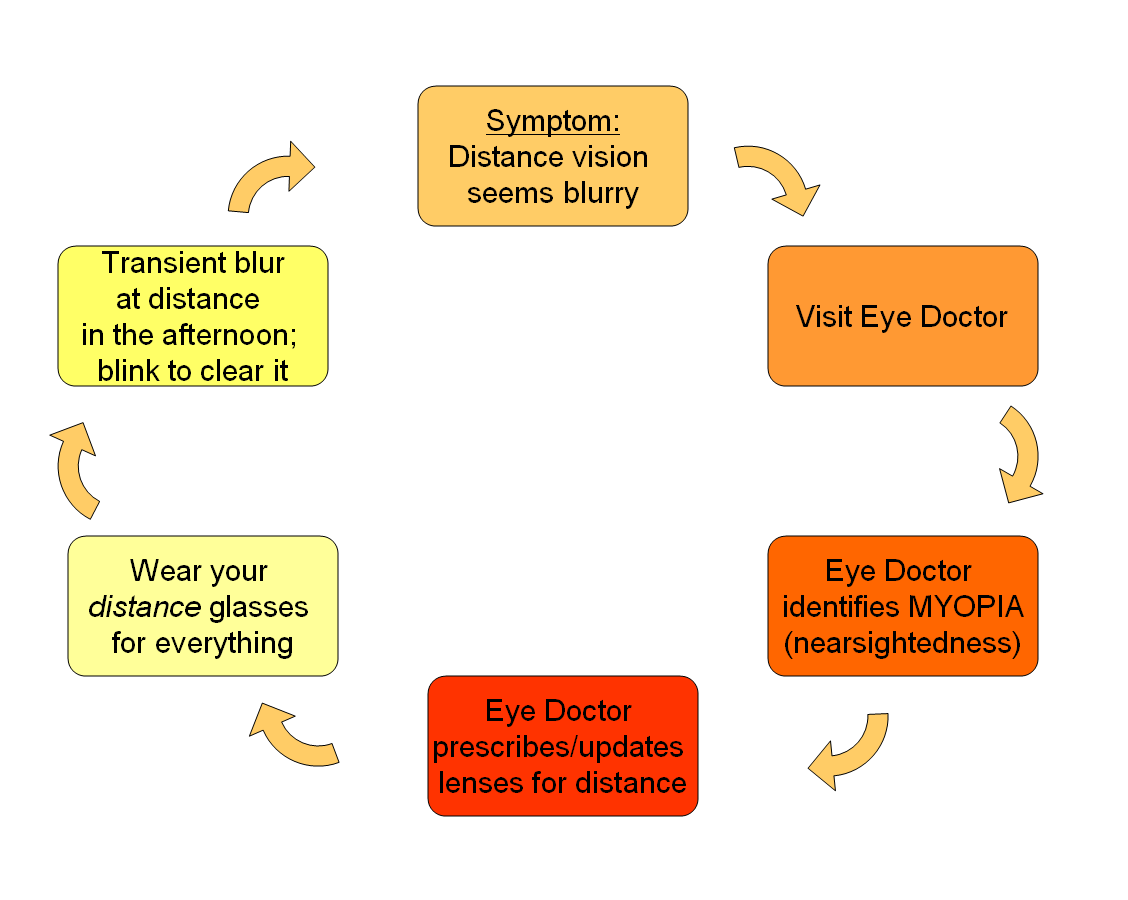
Once the cycle begins, it tends to continue. It’s a rarity that a young person (who can focus for near) is prescribed distance glasses and uses them only for distance viewing. That is the only gateway out of the cycle for most early myopes!
The cycle continues…
There is a very simple reason why this familiar problem becomes a cycle:
The solution (distance glasses) REGENERATES THE PROBLEM!
The “catch” is, most people do not simply go near-sighted because it is in the genetic code. Yes, there may be a genetic predisposition, but both nature and nurture play a role in what ultimately comes to pass.
Why does the cycle continue?
It’s a simple explanation:
We are highly adaptive beings.
When we have a need, we adapt ourselves to best suit that need.
For people who spend a great deal of time engaged in near-point work, their visual system re-organizes so that near-point work can be done with reduced effort. The “resting point” of the visual system shifts from all distances at-ease (called “emmetropia“, see section below) to better comfort at near-point (early myopia).
When you develop myopia, you give yourself a “head start” for focusing at near-point (think of this as a base-runner taking a lead off the first-base bag in order to shorten the distance to second base), while leaving your distance viewing “clear enough” so that you can get around. The more time you engage in distance viewing activities (like sports), the less likely you are to sacrifice the quality of your distance vision.
So, how do the distance glasses regenerate the problem?
Very simple:
It resets your focus for full distance… and simultaneously makes near-point viewing more effortful!
Again, as a highly adaptive being, when you are engaging in prolonged, intense near-point work, you often re-adapt the SAME SOLUTION you did before, re-biasing yourself to see at near-point with less effort.
Therefore, by the next visit to the eye doctor, your prescription has gone up from -0.50 (the first step into myopia) to -1.00. You have re-adapted the same -0.50 on top of your previous -0.50!
The faster your prescription gets updated, the faster the cycle propels itself into higher and higher levels of myopia!
Breaking the cycle…
When does the cycle stop?
If you ask most nearsighted adults, they will tell you:
- “Shortly after I graduated college…” or
- “It began when I went into law school/ grad school/ med school… and stopped after the intensive studies stopped…”, or
- “I still read intently all the time… the nearsightedness continues to increase….”
Alternatively, there IS a way to break the cycle! Simply TREAT THE UNDERLYING PROBLEM!
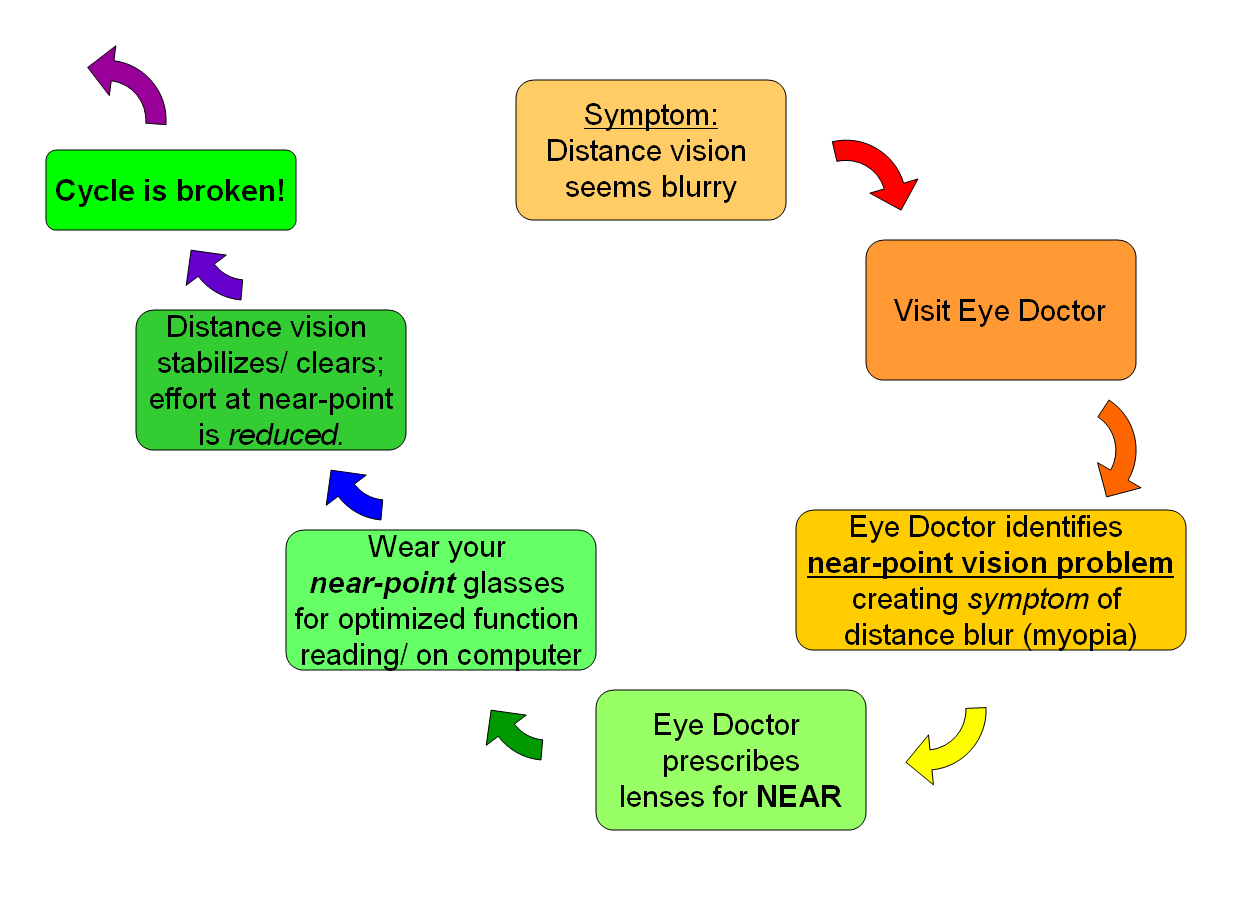
Prescribing lenses for near-point can be done in several different ways:
- Reading glasses
- Bifocals
- Reading glasses over distance contact lenses
- Multifocal contact lenses (which have been shown to slow myopia progression)
This solution addresses the UNDERLYING Near-point Vision Problem, which may take more time and careful testing than simply treating the symptom or complaint of distance blur. Doctors who take a Behavioral or Developmental approach to optometry will often do testing and treatment of near-point vision problems during a comprehensive eye and vision exam. Often, this includes private offices, where a “family practice” cares for children as well as adults. The difference is time– these problems are not identified and treated in most 15 minute encounters.
Wondering if it really is nature or nurture? Read on, to see what is the likelihood of myopia vs emmetropia.
Emmetropization
Emmetropia is a very mild degree of farsightedness, leaving just a small buffer in the focusing system so that distance viewing does not require complete visual relaxation. It’s a way that a person can keep the visual system engaged and poised for re-focusing at any distance. (Think of this as an athlete that is warmed up for their event– maximally flexible and actively engaged, rather than straining to fully relax or rest any of their muscles.) The vast majority of humans develop emmetropia from a state of relative farsightedness in the first few years of life. This process is called emmetropization. In the natural course of visual-motor development, an active and balanced visual system varies viewing between distance and near-point objects, which is best served by an emmetropic refractive state.
A look at the epidemiological spread of Refractive States (“eye powers”) shows how most people are likely to develop emmetropia. If vision development did not shape our refractive states, this curve would be more bell-shaped or evenly distributed throughout the eye-powers.
Myopia is a great concern in China, as the development of myopia appears to be epidemic.
The following study of chilren’s refractive development in Western China demonstrates how experience with intensive education gradually tips the scales in the direction of myopic development:
Frequency histograms of spherical equivalent diopter data for (A) children in 6-8-year-old group (n=891), (B) 9-12-year-old group (n=1315), and (C) 13-15-year-old group (n=864). Values on the x-axis represent spherical equivalent diopter. The interval of each column is 0.25 D. Data were from the left eyes of 3070 school-age children.
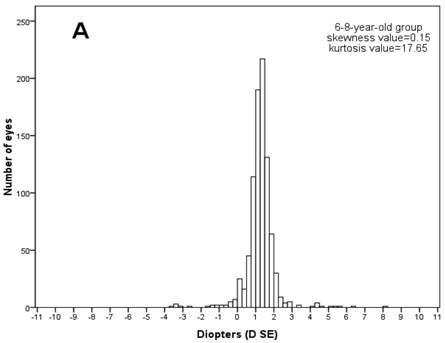
Notice that the early ages are mildly biased to farsightedness (hyperopia), with (+) refractive powers
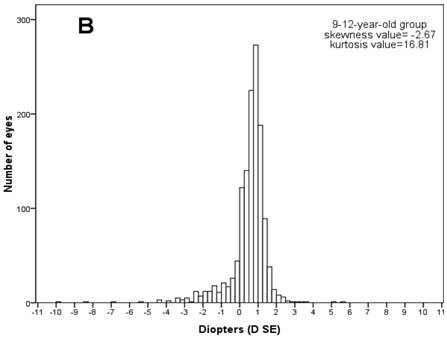
The basic refractive state shifts from hyperopic to emmetropic (between 0-1 D).
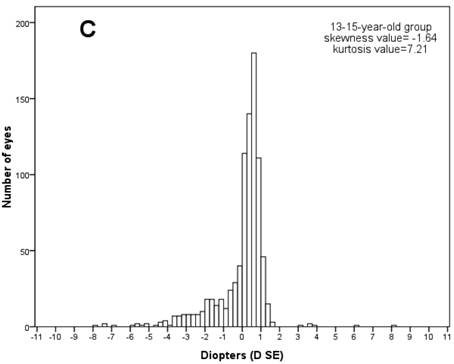
As children age and engage in more academic work, there is also an increase in the number of children with myopia (<0 D).
(From Pi LH, Chen L, Liu Q, Ke N, Fang J, Zhang S, Xiao J, Ye WJ, Xiong Y, Shi H, Yin ZQ. Refractive Status and Prevalence of Refractive Errors in Suburban School-age Children. Int J Med Sci 2010; 7(6):342-353. doi:10.7150/ijms.7.342. Available from http://www.medsci.org/v07p0342.htm)
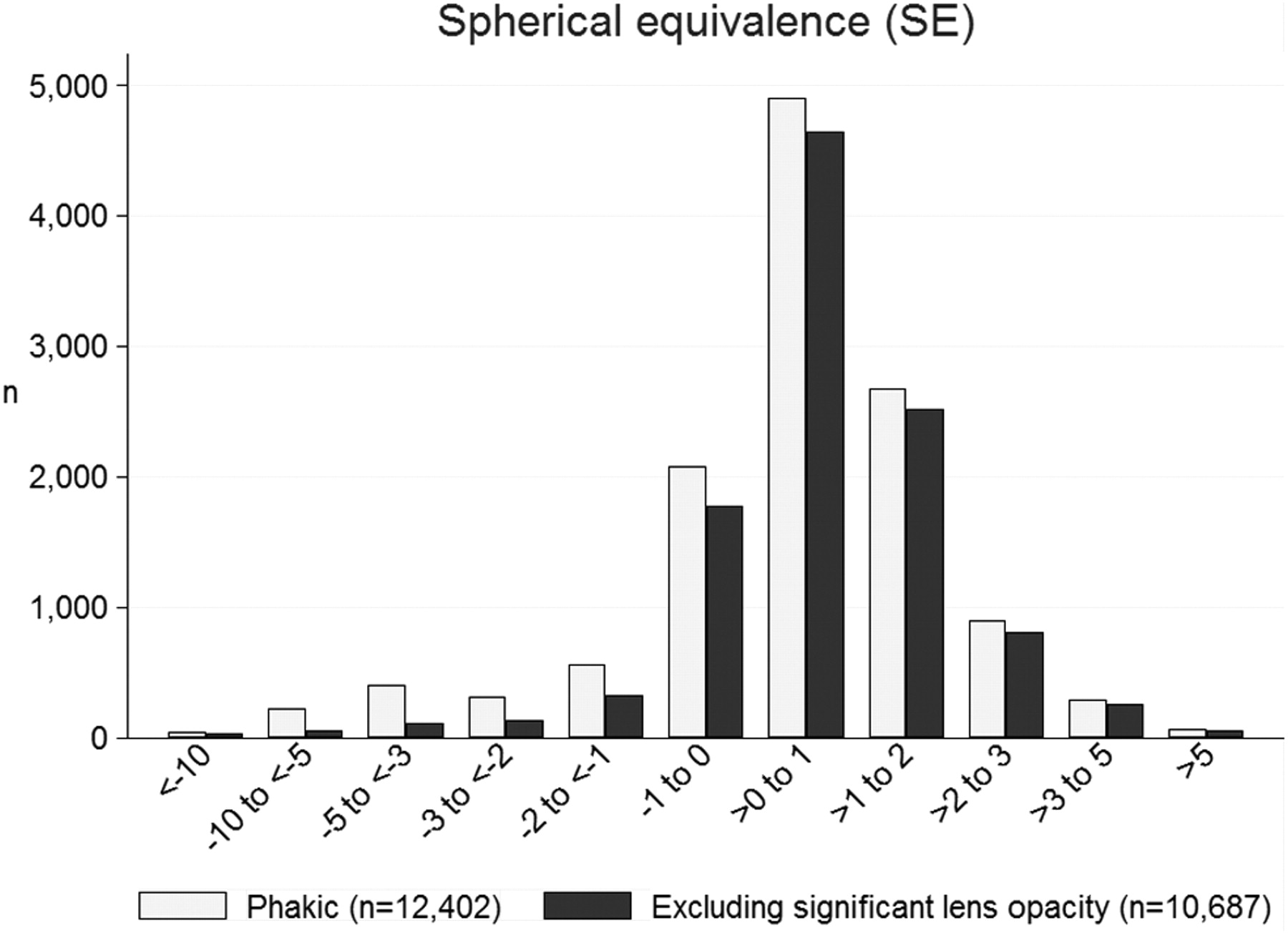
In this study of over 10,000 participants in Nigeria, the vast majority of refractive states is between -1 D and +2 D; Those with emmetropia (between 0 and +1 D) outnumber all other groups by a factor of 2. Source article: http://iovs.arvojournals.org/article.aspx?articleid=2187823 Ezelum et al; Nigeria National Blindness and Visual Impairment Study Group. Refractive Error in Nigerian Adults: Prevalence, Type, and Spectacle Coverage. Investigative Ophthalmology & Visual Science July 2011, Vol.52, 5449-5456. doi:10.1167/iovs.10-6770
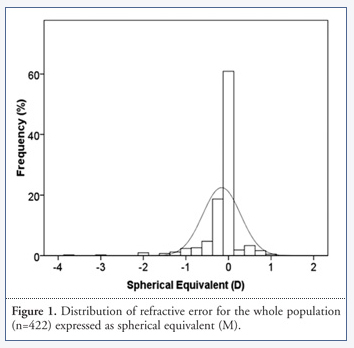
This image shows the pointed skewing of refractive states just around the 0 D power in a study in Mozambique, with 422 subjects. Compare the bar graph with the Normal-distribution curve, to see how much more common emmetropia is than other refractive states. From: http://www.journalofemmetropia.org/2171-4703/jemmetropia.2011.2.137.141.php Alcocer, et al. Prevalence of Refractive Error in Young Urban Students in Mozambique. J Emmetropia 2011; 2: 137-141.
Questions and comments? Please share your thoughts!
And, if this helps “clear things up” for you, please share the information for others!
I am just slightly nearsighted, and wear -.50 for each eye. I wear the glasses full time for distance, reading, and computer work.
I love the super sharp vision, and minification that that they give me.
I also have a pair with -.75, a slight over correction, that I wear if my eyes feel fatigued.
My prescription has not increased in ten or more years, but when I first got the glasses, I could see fairly well without them, but now if I remove then my vision is very blurred, at any distance.
Hi Dale,
My apologies for the delayed reply.
Your comments suggest that you have increased your degree of myopia through a habit of over-compensating your myopia.
Your focusing system may have become less flexible over time (which is common and expected), and you do not have the flexibility now which you used to enjoy. That may explain why you used to be able to wear the over-powered lenses without an increase in myopia, but that this is no longer the case.
Please consider that when you add the (-0.75) lenses over your near-point demands, which may require focusing skills of +1.50 to +2.50 D, you are indeed over-compensating.
For example, if you were truly a -0.75D myope, to see at a demand of 2.00D (at a 50 cm distance), you would need to exert only 1.25D of focusing effort with your glasses OFF. You would need to exert 2.00D of focusing effort with your glasses ON.
I would encourage you to try reading and computer work without your glasses for now. It would be equivalent to having a low reading prescription for a person who is not near-sighted. You may even enjoy less distance blur once more.
Best wishes!
Dr. Slotnick
Thank you for getting back to me Dr.Slotnick.
I called my optometrist to discuss this, and learned that I actually am not myopic, but he has me wearing this prescription because I have -1.50 of astigmatism in each eye, and can not tolerate the cylinder lenses to correct it.
Thinking back to the first glasses that he gave me more than ten years ago because I had blurred vision at any distance were cylinder lenses. Vision with these glasses gave me headaches, and reading with them for any extended time was clear, but when looking off into the distance everything was blurred. When he gave me the -.50 glasses that problem went away.
He refers to my prescription a spherical equivalent prescription.
I understand, Dale. In our practice, we often modify the lenses compared to the measurements with an interest in comfort and wearability. Sounds like your doc found a clever solution for you. If you can follow my previous comment, it still applies. Best wishes! -Dr. Slotnick